INTRODUCTION
In the cardiac arrhythmias genesis intervene two fundamental physiopathological mechanisms: the impulse formation dysfunctions and the conduction of these impulse dysfunctions. Among the conduction of the impulse dysfunctions we have the auriculoventricular (AV) blockades and the intraventricular (IV) blockades, which have great significance due to the graveness of the clinical presentation, as well as the complexity of the therapy to use. In this therapy where there are always two alternatives to analyze: the pharmacological resynchronization therapy or the therapy by the installation of cardiac resynchronization devices(1).
For the diagnose of the arrhythmias, sometimes with the simple 12 derivations electrocardiogram is enough, nevertheless, some require advanced electrophysiological studies, invasive or not(2), that give us tools for the diagnosis of mixed conduction dysfunctions, like it is the case of the one presented in this article.
The prolongation of the QRS complex due to complete and incomplete left bundle branch blockades is a factor of high importance for systolic heart failure(2). The heart resynchronization therapy that includes the installation of a cardiac resynchronization device provides clinical benefits for patients suffering these pathologies(3).
Complete left bundle branch blockades (LBBB) can be associate to other blockades, those can be AV or IV. The clinical manifestations and the degree of severity will be in correspondence with the place of the blockade, either suprahisian or infrahisian(4). The concurrence of blockades at several levels is always difficult to handle with, and its evolution is potentially fatal if accurate measures are not taken. The complexity of the diagnosis of this type of multiple blockades makes registered experiences of these cases very rare in the literature.
CASE REPORT
A 65 year-old white retired female patient, came to the Emergency Room complaining of severe and oppressive chest pain, which showed up suddenly, irradiated to the left jaw and shoulder, accompanied by increasing dyspnea. As past medical history, she admitted suffering from hypertension for the last 30 years and ischemic cardiophaty since she was 45 years old. She also admitted isolated decompensating crises of her base illnesses along the years. The patient was also obese.
On physical examination it was verified that the patient was anxious, with accused dyspnea, in orthopnea, pale and with presence of outlying cyanosis. The heart beats were rhythmic, with good tone and intensity, however there was not listen murmur, neither third or fourth heart noises. Isolated crackles were auscultated in both lung bases. The vital constants showed: heart rate: 112 beats per minute, breathing frequency: 26 respirations per minute and the blood pressure was high at 170/110 mmHg. It was also carried out a simple chest X-Ray, in decubitus supine, showing slight increase of the cardiothoracic index.
The
following tests were indicated: hemoglobin (12,6 g/L), global count of
leukocytes (9,2 x 109/L), glycemia (7,6 mmol/L), creatinine (78 mmol/L), CPK
(55 U/L) and CPKMB (12 U/L). A twelve derivations electrocardiogram (picture 1) was carried
out with a Cardiocid D200A equipment, at 25 mm/seg (picture 1) showing sinus
rhythm, left axis, elongate PR segment (0,28 seg) consistent with a first
degree auriculoventricular blockade, wide and aberrant QRS complex (0,20 seg)
in all the derivations consistent with LBBB, besides qS complex with R wave
beheaded and ST segment elevation of 2 mm in DIII, qS complex with R wave
beheaded and ST segment elevation of 3 mm in aVR. Moreover ST segment
relegation of 2 mm in DI, DII, aVL and V4.
After being compared with previous EKG, it was recognize as new pattern and it was diagnose as an acute coronary syndrome with ST segment elevation, according to the existent protocol implemented in our service. Invasive monitoring was applied, internal jugular central vein was channeled by posterior way, general support measures were applied and pharmacological coronary reperfusion therapy was establish.
The patient suffered a tragic evolution. The monitor showed isolated ventricular extra systoles, which were progressively modified toward the presentation of torn pieces of ventricular tachycardia (VT). Eventually the patient fell in cardiac arrest, and despite the advanced cardiopulmonary resuscitation maneuvers the patient didn't revert to spontaneous circulation. Death was declared.
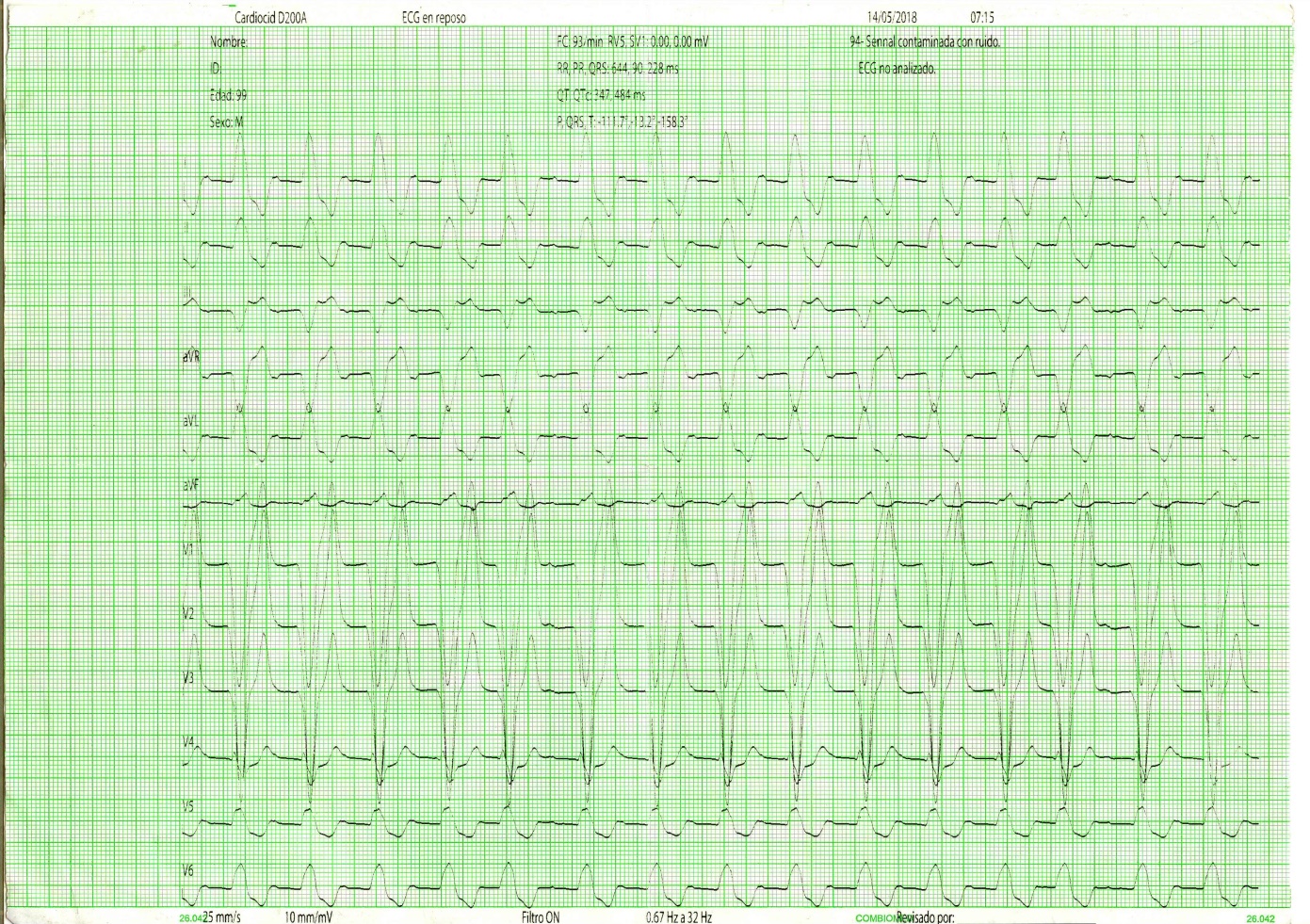 Picture
1. EKG with LBBB associated to Blockade AV of 1st degree
Picture
1. EKG with LBBB associated to Blockade AV of 1st degree
DISCUSSION
The cardiovascular illnesses is coming in general population, with independence of sex, increasing considerably with age, until reaching the 14 % of the world population between the 6th and 8th decades of life(5).
Specifically our country has shown an ascent in the presentation of these cardiovascular events, showing the statistical annuals that in the year 2000 the rate of mortality was of 181,1 for each 100 thousand inhabitants, in the year 2016 the rate of mortality was of 217,4 for each 100 thousand inhabitants and in the year 2017 was of 241,6 for each 100 thousand habitants(6).
These data reflects the marked increase of these entities in our population, being the heart illnesses those that occupy the first place regarding the number of deaths per year. Among their diverse presentation forms, it is the Ischemic Cardiophaty the one that registers bigger mortality around the world every year, independently of the region(6).
The AV or IV blockades have extensive presentation, which can appear asymptomatic if the escape rhythm is appropriate, or to have serious presentation showing a period of asystole, until an escape rhythm appears, causing a typical syncopate scene called Stokes-Adams crisis(4).
This association of LBBB with 1st grade AV blockade has been described previously in diverse case presentations, being related to rheumatic illness, Sjögren Syndrome, among others(7,8).
Trifascicular blockades, as the one previously described, have been mainly described associated to a LBBB with AV blockade of high grade, such as 2nd degree, either in Mobits type 1 form or type 2, or 3rd degree AV blockade.
Nowadays as combined treatment of this association of IV and AV blockades, the installation of self-defibrillation pacemaker is indicated, unfolding three spikes: one to the right atrium, another in the Sheaf of His, and a third in the right ventricle, achieving this way the synchronous depolarization from both ventricles to the unison, effect that previously was not achieved with other techniques(9,10).
CONCLUSIONS
Trifascicular
blockades can be shown as fatal complications of ischemic cardiophaty. The
auriculoventricular or intraventricular blockades have extensive presentation
population between the 6th and 8th decades of life. If
the suitable therapy does not settle down prematurely the patient's outcome
it’s affected drastically.
CONFLICT OF INTERESTS
The authors declare that does not exist an
interest conflict.
AUTHOR CONTRIBUTION
All
authors participated in the writing of the article, its review and approval of
the final version.
FINANCING
The authors did not receive
funding for the development of this article.
BIBLIOGRAPHIC REFERENCES
1. Libby P, Bonow RO, Zipes DP, Mann DL, Braunwald E. Braunwald. Tratado de Cardiología. Texto de Medicina Cardiovascular. Madrid: Elsevier; 2009
2. Elsayed YMH. Acute myocardial infarction associated with right bundle branch block and changeable trifascicular block: a case report. J Acute Dis [Internet]. 2019 [cited 2019 Jun 10]; 8 (5): 215-220. Available at: http://journals.hainmc.edu.cn/jad/article/abstract/20190508
3. Prinzen FW, Vernooy K, Auricchio A. Cardiac resynchronization therapy. State-of-the art of current applications, guidelines, ongoing trials, and areas of controversy. Circulation [Internet]. 2013[cited 2019 Jun 15]; 128: 2407-18. Available at: https://www.ahajournals.org/doi/full/10.1161/circulationaha.112.000112
4. Rozman C, Cardellach López F. Farreras Rozman. Medicina Interna [Internet]. 18 va ed. Barcelona, España: Elsevier España, S.L.U.; 2016 [cited 27 Nov 2017]. Available at: https://www.clinicalkey.es/#!/content/book/3-s2.0-B9788490229965000557
5. Noya Chaveco ME, Moya Gonzáles NL. Roca Goderich Temas de Medicina Interna. 5ta ed. La Habana, Cuba: Editorial de Ciencias Médicas; 2017. pp 447-58.
6. Ministerio de Salud Pública. Dirección de Registros Médicos y Estadística de salud. Anuario Estadístico de Salud 2018. [Internet]. 2019 [cited 2019 Feb 20]. [approx. 193 p.]. Available at: http://files.sld.cu/dne/files/2019/05/Anuario-2018-Ingles-compressed.pdf
7. Jobling K, Rajabally H, Ng WF. Anti-Ro antibodies and complete heart block in adults with Sjögren’s syndrome. Eur J Rheumatol [Internet]. 2018 [cited 2019 Sep 10]; 5 (3): 194-6. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6116846/
8. Nadine A, Daniel K, Ahran A, Shun-Shin M, Whinnett ZI, Sohaib A. His Bundle Pacing: A New Frontier in the Treatment of Heart Failure. Arrhythm & Electrophysiol Review [Internet]. 2018 [cited 2019 Nov 15]; 7 (2): 103–10. Available at: https://doi.org/10.15420/aer.2018.6.2
9. Tan AWX, Ho KL, Ching CK, Chua KCM. An implantable cardioverter defibrillator in a patient with triple mechanical valves. Clin Case Rep. 2018 [cited 2019 Sep 05]; 6 (9): 1795–1800. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6132153/
10.
Hideyuki Hasebe. A Patient with Left Bundle Branch Block and Persistent Atrial
Fibrillation Treated with Cardiac Catheter Ablation and Pharmacologic Cardiac
Resynchronization Therapy without the Use of an Implantable Cardiac Device. Am
J Case Rep [Internet]. 2018 [cited 2019 Aug 29]; 19:
123-127. Available at: https://www.amjcaserep.com/abstract/index/idArt/907268
Author notes
cralmirag@infomed.sld.cu





