Importanceof theevaluationofthequalityof lifein bariatricsurgery
Importancia de la evaluación de la calidad de vida en cirugía bariátrica
Mexican Journal of Medical Research ICSA, vol. 8, no. 15, 3-8, 2020
Universidad Autónoma del Estado de Hidalgo
Articles
Received: 06 March 2019
Accepted: 30 August 2019
Published: 05 January 2020

Abstract: Obesity is a serious health problem that has increased in recent decades. It is a chronic disease responsible for serious physical, psychological and social problems, reaching to alter the quality of life of people who suffer from it. Bariatric surgery is the best treatment for obesity even in its most severe levels, since in addition to reducing excess weight, it achieves a high rate of improvement and remission of metabolic comorbidities, improving the quality and expectation of life of the operated patients. Within bariatric procedures, laparoscopic gastric bypass and laparoscopic sleeve gastrectomy are the most performed worldwide. Quality of life is defined as, the perception that the obese person has of their physical, psychological, and social limitations and the reduction of opportunities. The success of the surgery consists of changing the quality of life of the patient. The results should not be evaluated only according to the initial loss or late weight gain, complications or sequelae of one or another technique or the subsequent need for cosmetic surgery, but a series of factors derived from the patients themselves should be taken into account, which together define the quality of life and even the cost / benefit ratio.
Keywords: Bariatric surgery, quality of life, obesity.
Resumen: La obesidad es un grave problema de salud que ha ido incrementado en las últimas décadas. Es una enfermedad crónica responsable de graves problemas físicos, psicológicos y sociales, llegando a alterar la calidad de vida de las personas que la padecen. La cirugía bariátrica es el mejor tratamiento para la obesidad aún en sus grados más severos, ya que además de reducir el exceso de peso, logra una alta tasa de mejoría y remisión de las comorbilidades metabólicas, lo que incide en mejorar la calidad y expectativa de vida de los pacientes operados. Dentro de los procedimientos bariátricos, el bypass gástrico laparoscópico y la manga gástrica laparoscópica son los que más se realizan a nivel mundial. La calidad de vida, es definida como, la percepción que la persona obesa tiene de sus limitaciones físicas, psicológicas, sociales y a la disminución de oportunidades. El éxito de la cirugía consiste en el cambio de la calidad de vida del paciente. Los resultados no deben valorarse sólo según la pérdida inicial o ganancia tardía de peso, complicaciones o secuelas de una u otra técnica o la necesidad posterior de cirugía estética, sino que debe tenerse en cuenta una serie de factores derivados del propio paciente que, en conjunto, definen la calidad de vida e incluso la relación costo/beneficio.
Palabras clave: Cirugía bariátrica, calidad de vida, obesidad.
INTRODUCTION
Obesity is a serious health problem that has increased in recent decades. It is a chronic disease responsible for serious physical, psychological and social problems, reaching to alter the quality of life (QL) of people who suffer from it.1 It is constituted as a chronic pathology, which presents not only a higher mortality but also comorbidity, in relation to its severity,2 associated with cardiovascular diseases and their risk factors, such as hypertension, dyslipidemia and glucose intolerance.3 Bariatric surgery is the best treatment for obesity even in its most severe levels, since in addition to reducing excess weight, it achieves a high rate of improvement and remission of metabolic comorbidities, which favors the quality and expectation of life of the operated patients.4 It is necessary that the health professional has a thorough knowledge of the disease and its complications, as well as the existing options for its treatment; from the management of behaviors for the acquisition of a healthy lifestyle to drugs, nutrients and surgical options, in order to contain the impact it has on the years of healthy life, life expectancy and occupational health of individuals.5
Definition of obesity
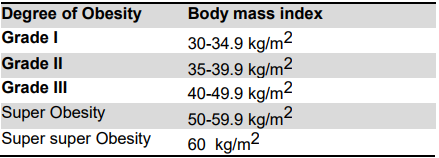
According to the World Health Organization (WHO), obesity is a chronic disease, characterized by an increase in body fat, associated with a greater health risk.6 The current classification of Obesity proposed by the WHO is based on the BMI, which is shown in Table 1, being the most useful measure for its diagnosis, since it is the same for both sexes and adults of all ages.7
Morbid obesity is defined as the disease characterized by the excessive increase of body fat, whose magnitude and distribution compromise the health of other organs and systems. It is distinguished by being chronic and multifactorial and is the result of an imbalance between the energy ingested and the energy expended.8 According to the National Institutes of Health of the United States, it is defined as an overweight of 50 to 100% over ideal body weight, or 45 kg over ideal body weight. The criterion of a body mass index (BMI) higher than 40 is also taken into account.9
Epidemiology of obesity
A search for "obesity epidemic" returns almost 8,000 articles in PubMed. Despite widespread attention, no country has successfully reversed its obesity epidemic. In 2013, the WHO proposed a Global Plan of Action for the prevention and control of non-communicable diseases, including obesity targets and indicators to monitor progress.10 Obesity has evolved as a pandemic disease, with an increase in its prevalence and severity. The main cause lies in the change in the lifestyle of modern society, which has generated a huge imbalance between energy consumption and expenditure.. Being a health problem throughout the world, considered one of the most serious and prevalent non-communicable diseases of the 21st century.11 An analysis of the epidemiological transition in Mexico found that chronic non- communicable diseases caused 75% of the total deaths and 68% of the years of life potentially lost. This epidemiological scenario allows us to measure the severity that obesity represents in Mexico and justifies the management of profitable and successful health programs and projects to solve this problem.7 There is higher mortality from any other cause, the more serious the obesity gets. The life expectancy of people with morbid obesity is reduced around 5 and 20 years depending on sex, age and race. The Organization for Economic Cooperation and Development places Mexico in the second place of obesity in adults globally, surpassing the USA. Some studies project that by 2050 there will be more people with higher obesity.8 The nutritional transition experienced by the country has as characteristics a westernization of the diet, specifically:
1) increase in the availability at low cost of processed foods added with high amounts of fats, sugar and salt; 2) increase in the consumption of fast food; 3) decreased time available for preparing food at home; 4) an important increase in the exposure of advertising and supply of industrialized foods, and 5) an important decrease in the physical activity of the population. The current situation of overweight and obesity in Mexico requires implementing a comprehensive policy, multisectoral and with effective coordination, to achieve changes in eating patterns and physical activity that allow the prevention of chronic diseases and reduces the prevalence of overweight and obesity.7
Definition of bariatric surgery
The term “bariatric surgery” derives from the Greek root “baros”, which means relative to weight; therefore, bariatric surgery defines the set of surgical interventions designed to produce significant weight loss.12 It is an effective surgical procedure performed on the stomach and / or intestines that helps to lose weight in a person with morbid obesity. It allows a complete resolution or improvement of the following clinical conditions: diabetes mellitus, hyperlipidemia, systemic hypertension and obstructive sleep apnea.13It should be carried out in a center of high experience and with the participation of a multidisciplinary team to maintain low morbidity and mortality, prevent and treat early complications, reinforce adherence to post-operative indications and change the permanent lifestyle, essential to maintain the effects of bariatric surgery.4 While surgeons have been refining the role of gastrointestinal operations for the treatment of obesity for more than 60 years, for the first time, the American Diabetes Association 2017 Standards of Medical Care includes specific guidelines that make metabolic surgery part of the standard care of diabetic patients.10
Bariatric Surgery Techniques
The laparoscopic gastric bypass of Roux-en-Y, involves the creation of a small gastric reservoir (15-20 mL) which is separated from the remaining stomach, the gastric reservoir is connected by a small and calibrated anastomosis to a Roux-en-Y, member of the jejunum, therefore, it does not pass through the duodenum and the proximal jejunum. The laparoscopic sleeve gastrectomy consists of a vertical resection of 70% of the stomach that leaves a narrow longitudinal tubular gastric reservoir where the flow of nutrients through the duodenum and small intestine remains intact. The biliopancreatic diversion with change is a more complex process, which implies a reduction of the gastric capacity and a more extreme duodenal, leaving a small and relatively short intestinal bypass for the absorption of food. Adjustable gastric band is a silicone collar with an inflatable component, which surrounds the upper stomach and connects to a subcutaneous port to adjust the band size.14 Within bariatric procedures, laparoscopic gastric bypass (LPGG) and laparoscopic gastric sleeve (LMW) are the most performed worldwide.15 The National Institutes of Health have concluded that bariatric surgery is an adequate therapy for patients who have failed to respond to medical treatment.16 The gastric bypass achieves the best balance between results, complications and quality of life.17 It is considered that the quality of any bariatric surgical technique would be defined, in general terms, both by the reduction of overweight and its subsequent maintenance, by the cure or improvement of associated comorbidities, by the achievement of a correct "modus vivendi" and the lack of sequel.18
Bariatric operations are classified as malabsorptive, restrictive, or a combination of the two. Malabsorption procedures produce weight loss by interference with normal digestion and absorption. Restrictive procedures induce weight loss by limiting intake. Malabsorptive and restrictive mixed procedures produce malabsorption and limit the intake. Probably there are no true restrictive operations.10
Indication of surgical treatment
Bariatric surgery is performed more and more frequently in surgical services, due to various reasons: the exponential increase in pathological obesity with its associated important comorbidities, a greater involvement of the increasingly younger patient and the existing scientific evidence, which it supports that at present, only surgery allows an effective and continuous treatment over time, with the consequent benefits for patients even in cases of extreme obesity.17
According to the Official Mexican Standard, the indication for bariatric surgery is established in adult individuals with a BMI higher than or equal to 40 kg/m² or higher than or equal to 35 kg/m² associated with comorbidity, whose origin in both cases is not purely endocrine type. There must be a history of recent comprehensive medical treatment. In addition to the above, in the case of people aged 16 to 18 years, surgical treatment may be performed exclusively on those who have completed their physical, psychological and sexual development, in highly specialized medical care facilities, as part of research protocols, reviewed and approved by an Ethics Committee, under the care of multidisciplinary teams and only if they have important comorbidities. The indication of surgical treatment for obesity should be the result of the evaluation of a multidisciplinary health team, consisting at least of: surgeon, anesthesiologist, and internist, graduate in nutrition and clinical psychologist; this indication must be stated in a medical note.13
Quality criteria in bariatric surgery
The objectives of bariatric surgery are not always dependent on the selected technique, since this is largely influenced by the characteristics of the morbid obese (hence the importance of correct selection and adequate follow-up), any technique should meet the requirements stated by Baltasar et al.:19
1. Reliable, with a morbidity lower than 10% and mortality lower than 1%. 2. Effective, with losses of excess weight of more than 50% in more than 75% of patients at 5 years of follow-up. 3. Replicable technique, in such a way that the results of the different centers that perform it are comparable. 4. With revision percentages of less than 2% per year. Although this section only considers reoperations for causes derived directly from the intervention, it could also include instrumental interventions (gastroscopies, stenosis dilatations, etc.) that, although not involving a new surgical intervention, are necessary to treat sequel or complications of the procedure performed. 5. It offers a good quality of life, or that it does not alter it in a manifest way, due to the inability to make an adequate intake, the presence of recurrent vomiting or permanent diarrhea nonetheless, at least initially, and sometimes in the long term, the degree of patient satisfaction does not correlate with the changes induced in their quality of life, but in the long term, especially when there are severe restrictions on intake, lead to the patient boycotting the intervention. 6. With minimal side effects on organs or systems, the concept of which, as this surgery implies the possible appearance of such sequels, should at least be predictable, easily correctable or, better, avoidable and easily diagnosable. We must not forget that success in weight loss is directly related to the incidence of complications. 7. Easily reversible, although at this point the concept of functional reversibility should be included, aimed at defining the correction of intractable or serious sequel, as opposed to anatomical reversibility, which is sometimes impossible to achieve.19
The loss of overweight should always be combined with criteria of quality of life and safety, because an effective technique in weight loss may be discouraged, in practice, by late morbidity or important side effects that make it inadvisable.17
Quality of life
To determine the degree of well-being of a population, the concept of quality of life, originating from public health and medical ethics, was adopted, which alluded to the criteria for deciding on the advisability of especially painful, aggressive, radical treatments of high cost or still in the experimentation phase for patients, first and foremost, for terminal cases.20
The concept of quality of life (QL) currently incorporates three branches of science: economics, medicine and social sciences. Each of these disciplines has promoted the development of a different point of view regarding how it should be conceptualized.21 In the health field, it is especially important in the elderly, the chronically ill (such as those suffering from Morbid Obesity), and the terminally ill and disabled populations.22 Medicine associates it with the psychosomatic health of the organism, the functionality, the symptomatology or the absence of disease. The evaluation of QL is: (a) It is subjective, (b) the score assigned to each dimension is different in each person and (c) the value assigned to each dimension can change through life. In this context, it is important to highlight the need for some authors to incorporate evolutionary aspects in the specific evaluation of quality of life.21 The World Health Organization has defined the quality of life as the individual perception of one's position in life within the context of the cultural system and values in which one lives and in relation to its objectives, hopes, norms and concerns.20
Quality of life in bariatric patients
The success of the surgery consists in the change of the quality of life of the patient.23 The quality of life related to the health of the obese is affected in at least four aspects: 1) Problems directly related to excess body fat, which condition both physical problems (alteration of physical performance), mental (alteration of self-esteem, depression) or social (alteration of the relationship with others, social integration, sexual relations, etc.). 2) Problems related to complications derived from obesity, such as arthropathies, diabetes mellitus, arterial hypertension or arteriosclerosis. 3) Problems related to the vital prognosis and its perception, such as the expectations of suffering cardiovascular diseases or hypertension in the future, due to the awareness of obesity as a cardiovascular risk factor. 4) Changes in the quality of life related to health due to the results of a generally long treatment, slow results and frequent recurrences. Therefore, the traditional measures of morbidity and mortality are added and complemented with the assessment of quality of life, because the goal is not aimed at the elimination of the disease but to improve the quality of life related to the health of the patients during survival time.22
Bariatric surgery has a highly favorable impact on the quality of life and sexual function of men and women. In women, the improvement of desire was clear, and in men in the severity of sexual dysfunction.25
Another aspect that is little taken into account is how the type of surgical technique used affects the quality of life related to health. Therefore, it is necessary to carry out more longitudinal studies based on the studies carried out, which allow us to know the factors that influence the quality of life related to the health of patients with morbid obesity after bariatric surgery.26 The QL is understood as a subjective perception, influenced by their state of health and the ability to perform those important activities in the patient´s life. Quality of life is defined as, the perception that the obese person has of their physical, psychological, and social limitations and the reduction of opportunities. The study carried out by Fernández et al. shows that the area that improves most is social interactions, followed by work and physical activity areas, self-esteem and nutrition, and finally, sexual relations, 2 to 5 years after the bariatric surgery.27
Quality of life measurement instruments in bariatric patients
The most used questionnaire to evaluate the benefits of bariatric surgery is the evaluation system using the score Bariatric Analysis and Reporting Outcome System (BAROS) proposed by Oria and Moorehead in 1998.24 It has been validated as the best comprehensive evaluation system and objective of the benefits of bariatric surgery, since it considers different variables such as the loss of overweight, correction of diseases associated with severe obesity, morbidity and mortality of the procedure in the short and long term, and above all incorporates the assessment of postoperative quality of life;25 from this last instrument comes the Moorehead-Ardelt Test that evaluates 5 dimensions: self-esteem, physical activity, social relations, work and sexual performance,26 the Spanish version of this instrument, adds a sixth dimension that takes into account the food habits.22
The Inventory of Quality of Life and Health evaluates the quality of life in patients with any chronic or acute condition and with sensitivity to interventions. It consists of 53 multiple-choice items with a Likert- type scale consisting of response options from never to always, which evaluate 11 areas of life, focusing on: Deterioration in quality of life: concerns, isolation, body perception, cognitive functions, attitude towards treatment, free time, daily life and medical dependence. Quality of life: physical performance, family, social networks and relationship with the doctor. Perception of total quality of life. The scores of each reagent are obtained by direct summation, where 0 is equal to never, 1 to almost never, 2 to a few times, 3 to frequently, 4 to almost always and 5 to always. The scales physical performance, family, social networks and relationship with the doctor are scored backwards. The instrument shows internal consistency (alpha coefficients range from 0.6831 to 0.9337) and adequate concurrent validity.28
The effect of bariatric surgery on quality of life is not entirely clear, there being many covariates that can affect the quality of life of people with morbid obesity.26 The quality of life two years after the intervention improves especially in physical aspects compared to the mental ones. It would be interesting to analyze some of the socio- demographic aspects, which could help in the identification of potential psychological problems that arise after surgery, favoring patient follow-up and adherence to postoperative protocols.29 It has been observed that those patients that undergo plastic surgery after bariatric surgery have better quality of life improvements compared to those who do not.30 The results should not be evaluated only according to the initial loss or late weight gain, complications or sequel of one or another technique or the subsequent need for cosmetic surgery, but a series of factors derived from the patient itself should be taken into account, define the quality of life and even the cost / benefit ratio.19 The use of the quality of life assessment questionnaire should be formalized to all patients in weight reduction programs that are clinical or surgical in order to measure and compare the results not only at an institutional level but also in all centers that perform bariatric surgery.31
CONCLUSION
The evaluation of quality must be done before and after bariatric surgery, as part of the integral assessment of the patient, since the importance is to obtain fundamental information from the patient's perspective. Currently, weight loss is considered only as a parameter of success in surgery, without involving other factors that condition success and improvement in their quality of life.
REFERENCES
1. Alcaraz García AM, Ferrer Márquez M, Parrón Carreño
2. Cabrerizo L, Rubio MÁ, Ballesteros MD, Moreno Lopera, C. Complicaciones asociadas a la obesidad. Rev. Esp. Nutr. Comunitaria. 2008;14(3):156–62.
3. Delago Floody P, Caamaño Navarrete F, Jerez Mayorga D, Campos Jara C, Ramírez Campillo R, Osorio Poblete A, et al. Efectos de un programa de tratamiento multidisciplinar en obesos mórbidos y obesos con comorbilidades candidatos a cirugía bariátrica. Nutr. Hosp. 2015;31(5):2011–6.
4. Karin Papapietro V. Cirugía para la Obesidad: Efectos generales, beneficios y riesgos. Rev. Med. Clin. CONDES. 2012;23(2):189–95.
5. Perea-Martínez A, López-Navarrete GE, Padrón-Martínez M, Lara-Campos AG, Santamaría-Arza C, Ynga-Durand MA, et al. Evaluación, diagnóstico, tratamiento y oportunidades de prevención de la obesidad. Acta Pediátr. Mex. 2014;35(31):316–37.
6. Manuel Moreno G. Definición y clasificación de la obesidad. Rev. Med. Clin. CONDES. 2012;23(2):124–8.
7. Dávila-Torres J, González-Izquierdo J de J, Barrera- Cruz A. Panorama de la obesidad en México Obesity in Mexico. Rev. Med. Inst. Mex. Seguro Soc. 2015;53(2):249–9.
8. Rivera Carranza T, Téllez Girón AL, Serna-Thomé MG. Tratamiento nutricional en el paciente con superobesidad y bypass gástrico en Y de Roux. Nutr. Clin. Med. 2017; XI (1):42–58.
9. Shiordia Puente J, Ugalde Velázquez F, Cerón Rodríguez F, Vázquez García A. Obesidad mórbida, síndrome metabólico y cirugía bariátrica: Rev. Mex. Cir. Endoscop. 2012;13(2):85–94.
10. Reavis KM, Barrett AM, Kron MD. The SAGES Manual of Bariatric Surgery. Segunda Edition. Editorial Springer. The SAGES Manual of Bariatric Surgery. 2018.
11. Barquera S, Campos Nonato I, Hernández Barrera L, Rivera Dommarco J. Evidencia para la política pública en salud. Obesidad en adultos : los retos de la cuesta abajo. ENSANUT 2012;2–5.
12. Maluenda GF. Cirugía Bariátrica. Rev. Med. Clin. CONDES. 2012;23(2):180–8.
13. Norma Oficial Mexicana NOM-008-SSA3- 2010, Para el tratamiento integral del sobrepeso y la obesidad. 2010;1–10.
14. Camacho D, Zundel N. Complications in bariatric surgery. Primera Edition. Editorial Springer. Laparoscopic Endoscopic Surgical Science. 2018. 1- 225.
15. Guilbert L, Joo P, Ortiz C, Sepúlveda E, Alabi F, León A, et al. Seguridad y eficacia de la cirugía bariátrica en México: análisis detallado de 500 cirugías en un centro de alto volumen. RGMX. 2018; XXX (XX):1–7.
16. Marshall JS, Srivastava A, Gupta SK, Rossi TR, Debord JR. Roux-en-Y Gastric Bypass Leak Complications. Arch. Surg. 2003; 138:520–524.
17. Carvajal-Balaguera J, García-Almenta MM, Delgado de Torres SO, Camuñas- Segovia J, Peña-Gamarra L, Fernández IP, et al. Bypass gástrico en el tratamiento de la obesidad mórbida y la superobesidad: estudio comparativo. Nutr. Hosp. 2007;22(5):607–11.
18. Importar imagenMenéndez P, Gambi D, Villarejo P, Cubo T, Padilla D, Menéndez JM, et al. Indicadores de calidad en cirugía bariátrica. Valoración de la pérdida de peso. Nutr. Hosp. 2009;24(1):25–31.
19. Baltasar A, Bou R, Del Río J, Bengochea M, Escrivá C, Miró J et al. Cirugía bariátrica: resultados a largo plazo de la gastroplastia vertical anillada ¿Una esperanza frustrada? Cir. Esp. 1997; 62:175-9.
20. Cardona AD, Agudelo GHB. Construcción cultural del concepto calidad de vida. Rev. Fac. Nac. Salud Pública. 2005;23(1):79–90.
21. Urzúa MA, Caqueo-Urízar A. Calidad de vida: Una revisión teórica del concepto. Ter. Psicol. 2012;30(1):61–71.
22. García-Almenta MM. Adaptación y validación española del Cuestionario de Calidad de vida de Moorehead- Ardelt II en pacientes obesos mórbidos e intervenidos de obesidad mórbida. Universidad Complutense de Madrid; 2018.
23. González Santamaría JR, Girón Márquez J, Limón Aguilar JL, Márquez Aldama G. Bypass gástrico. Tratamiento quirúrgico de la obesidad mórbida. Rev. Hosp. Jua. Mex. 2005;72(4):153– 60.
24. Oria H, Moorehead M. Bariatric Analysis and Reporting Outcome System (BAROS). Obes. Surg. 1998;8:487- 499.
25. González PJF, Gómez CG, Arriagada PG. Evaluación mediante score BAROS de los resultados del bypass gástrico en el tratamiento de la obesidad mórbida. Rev. Chil. Cir. 2006;58(5):365–70.
26. Moorehead MK, Ardelt-Gattinger E, Lechner H, Oria HE. The Validation of the Moorehead-Ardelt Quality of Life Questionnaire II. Obes. Surg. 2003; 13:684–92.
27. Fernández Rodriguéz M, Guerra Mora P, Martín Sánchez E, Fernández Rodríguez C. Calidad de vida en pacientes intervenidos de cirugía bariátrica. Nutr. clín. diet. hosp. 2016;36(3):106–13.
28. Vázquez Prado A, Montalvá Orón EM, De Tursi Ríspoli LC. Valoración de la evolución de las comorbilidades de la obesidad mórbida tras tratamiento quirúrgico mediante la técnica del cruce duodenal. Nutr. Hosp. 2007;22(5):596–601.
29. Catalán V, Salvador J, Frühbeck G, Gómez-Ambrosi J. Mejora en la calidad de vida tras cirugía bariátrica. An. Sist. Sanit. Navar. 2018;41(2):287–289.
30. van-der-Hofstadt Román CJ, Lea Costa C, Alonso Gascón MR, Rodríguez-Marín J. Calidad de vida en pacientes intervenidos de cirugía bariátrica. An. Sist. Sanit. Nava. 2018;41(2):291–2.
31. Barzallo Sánchez DE, Guadalupe Rodríguez RA, Flores Tamayo FH, Aguayo Vistín WG, Guadalupe Vallejo EN. Evaluación de la calidad de vida post cirugía bariátrica mediante la aplicación del score de baros en el Hospital General Enrique Garcés. Rev. Fac. Cien. Med. Univ. Nac. Cuenca. 2014;32(3):70-77.