

Articulos Originales
Histopathological characterisation of gallbladder cancer in the “Joaquín Albarrán” Hospital, Havana, Cuba, in the period 2010-2019
Caracterización histopatológica del cáncer de vesícula en el Hospital “Joaquín Albarrán”, La Habana, Cuba, en el periodo 2010-2019
Gaceta Médica Boliviana
Universidad Mayor de San Simón, Bolivia
ISSN: 1012-2966
ISSN-e: 2227-3662
Periodicity: Semestral
vol. 43, no. 1, 2020
Received: 25 September 2019
Accepted: 24 February 2020

Abstract:
Gallbladder cancer is a rare and highly lethal disease in the world.
Objective: To characterize histopathologically gallbladder cancer at the “Joaquín Albarrán” Clinical Teaching Surgical Hospital of Havana-Cuba, in the period 2010 to 2019.
Methods: A retrospective, descriptive and observational study was conducted, in which biopsy and necropsy records were reviewed to identify cases with a histological diagnosis of gallbladder cancer. Paraffin-embedded tissues from the archive were also reviewed.
Results: Ten cases of gallbladder cancer were diagnosed, nine female and one male, all over 60 years old. Histologically the predominant variety was moderately differentiated adenocarcinoma, being 2 of them mucoproducers, of which 1 was infiltrating and with lymphatic permeation.
Conclusion: Gallbladder cancer is a very low frequency disease and its diagnosis continues to be an incidental fact, that is, the diagnosis is established in the histopathological examination after cholecystectomy or in the necropsy. The most frequent variety is moderately differentiated adenocarcinoma.
Keywords: gallbladder, adenocarcinoma, infiltration.
Resumen:
El cáncer de vesícula biliar es una enfermedad poco frecuente en el mundo y altamente letal.
Objetivo: caracterizar histopatológicamente el cáncer de vesícula biliar en el Hospital Clínico Quirúrgico Docente “Joaquín Albarrán” de La Habana-Cuba, en el periodo 2010 al 2019.
Método: se realizó un estudio retrospectivo, descriptivo y observacional, en el cual se revisaron los registros de biopsias y necropsias para identificar los casos con diagnóstico histológico de cáncer de vesícula biliar, se revisaron además tejidos fijados en parafina del archivo.
Resultados: fueron diagnosticados 10 casos de cáncer de vesícula, 9 femenino y 1 masculino, todos mayores de 60 años. Histológicamente la variedad predominante fue el adenocarcinoma moderadamente diferenciado, siendo 2 de ellos mucoproductores, de los cuales 1 infiltrante y con permeación linfática.
Conclusión: el cáncer de vesícula biliar es una enfermedad con muy baja frecuencia y su diagnóstico, continua siendo un hecho incidental, es decir, que el diagnóstico se establece en el examen histopatológico luego de la colecistectomía o en la necropsia. La variedad más frecuente es el adenocarcinoma moderadamente diferenciado.
Palabras clave: vesícula biliar, adenocarcinoma, infiltración.
Gallbladder cancer (CVB) is a rare and highly lethal disease worldwide. In 1777, Maximillian de Stoll made the first description at the famous Vienna Clinic. Keen, in 1891, performed the first resection. In 1978, Piehler and Crichlow wrote the first large study of CVB showing a 5% survival rate (SV) in 5,835 cases analysed. As early as 1931, Garretón Silva highlighted the high frequency of CVB by describing that in a series of 350 patients with acute cholecystitis, 4 of them were affected by malignant transformation1.
Gallbladder neoplasia has low incidence rates in the United States and parts of Western European and Mediterranean countries2. However, in South America, high mortality rates have been reported, particularly in indigenous Chilean Mapuche, Bolivian and Hispanic Chileans (3.5-15.5 per 100 000)3.
In southern Peru, a proportion of 0.64% of patients with gallbladder cancer has been found among the total number of patients in a hospital in the region4.
In Cuba, it is not included among the top 10 malignant neoplasms5. It is rarely discovered only at the resectable stage and the median 5-year survival has remained for many years at 5-12% of cases, despite surgical intervention6.
These remarkable variations may be explained by differences in the prevalence of environmental exposures and genetic predisposition to carcinogenesis7.
High rates of gallbladder cancer are associated with insufficient access to health services including access to surgical services for cholecystectomy8; for example, in Chile the prevalence of cholelithiasis is 50% at the age of 50 years9, which is a known risk factor for gallbladder cancer.
Histopathologically, the vast majority of gallbladder neoplasms are adenocarcinomas (95-98%), with well or moderately differentiated forms accounting for 75-80% of them. The only histological type with a relatively favourable prognostic significance in terms of survival is papillary adenocarcinoma, with oat cell and adenosquamous carcinomas being the forms with the worst prognosis. Other histological types, of almost exceptional presentation, are: pure squamous cell carcinoma; granulosa cell tumour; embryonal rhabdomyosarcoma; carcinoid; carcinosarcomas; and tumours of haematopoietic or lymphatic lineage10.
The histopathological findings of CVB sometimes create diagnostic dilemmas, as it can mimic benign diseases, such as sinus Rokitansky-Aschoff sinus (RA), adenomyomatosis; therefore the diagnosis of CVB has some potential difficulties11.
The use of histological type and TNM staging are useful criteria for designing appropriate treatment and predicting survival in patients. The importance of clarifying the anatomopathological staging will have an impact on the future therapeutic decision, as encouraging results are currently being obtained with the radical surgical approach to gallbladder cancer4.
The prognosis for life in all stages of CVB is close to 5%. The median lifespan in incidentally diagnosed patients is 26.4 months12.
Given that in Cuba there is no high frequency of gallbladder cancer at the national level, we consider that the characterisation of a set of cases registered during the period 2010 to 2019 would be of great importance as it would allow us to establish a pattern of this type of lesion in a low-incidence population and thus contribute to establishing an alarm for gastroenterologists, surgeons and other specialists involved in the care of biliary-type manifestations, who should include the suspicion of gallbladder cancer as part of their thinking when faced with a patient with clinical symptoms of abdominal pain, dyspepsia, jaundice, among others.
Material and methods
A retrospective, descriptive and observational study was conducted from 2010 to 2019, in which the biopsy and necropsy records of the Department of Pathological Anatomy of the Hospital Clínico Quirúrgico “Joaquín Albarran’’ were reviewed to identify cases with a histological diagnosis of gallbladder cancer, then the reports were located according to the corresponding number in the case of biopsies and autopsy protocol in the case of necropsies.
The criteria taken into account for inclusion in the study were patients with a histological diagnosis of gallbladder cancer between 1 January 2010 and 20 June 2019.
Once the biopsy report and autopsy protocol numbers were obtained, the corresponding medical records were searched to obtain data such as age, sex, skin colour, pathological history, history of the disease, clinical manifestations, diagnosis, diagnostic procedures and treatments applied.
From the biopsy report and autopsy protocol, the histological type, degree of cell differentiation, degree of infiltration of the gallbladder wall or neighbouring organs were obtained, which data were used to establish the staging of the tumour, using the criteria established by the TNM System (tumour, lymph node and metastasis) of the American Joint Committee on Cancer (AJCC) in its 2018 version.
To obtain the microscopic images, the corresponding slides of each case were extracted from the histological library.
Results
In the 8-year period (1 January 2010 to 20 June 2019), 10 cases of primary gallbladder cancer were diagnosed histopathologically, of which six were findings from the study of cholecystectomy specimens (2186 cholecystectomies for calculous cholecystitis); one as a confirmation of the clinical diagnosis of gallbladder cancer with signs of jaundice; and three cases as an autopsy finding.
The distribution according to sex and age shows nine female cases and one male case, all over 60 years of age. The distribution according to skin colour shows that in the study group malignant neoplastic lesions of the gallbladder occur without a clear predominance according to race.
Of the total number of cancers diagnosed at the “Joaquín Albarrán” Clinical Surgical Hospital, gallbladder cancer accounted for 0.23% of malignant tumours. With regard to cholecystectomy as the primary surgical indication, CVB accounted for 0.32% of these. And for the group with incidental diagnosis at necropsy the frequency was 0.04% of autopsies.
100% of the cases had ultrasonographic studies describing vesicular lithiasis, which were corroborated in the macroscopic study of the surgical specimen.
Pathological findings
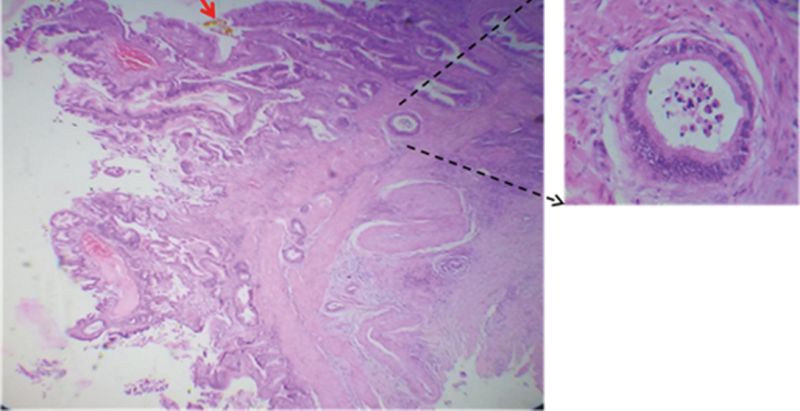
Of the 10 cases diagnosed with gallbladder cancer, 100% had a tumour that macroscopically had an exophytic vegetative appearance (Figure 1) and histologically corresponded to adenocarcinoma, with 20% being well differentiated (Figure 2) and 80% moderately differentiated. The mucinous variety was present in 40% of cases. Characteristically, one case had a papillary pattern with extensive tumour necrosis.

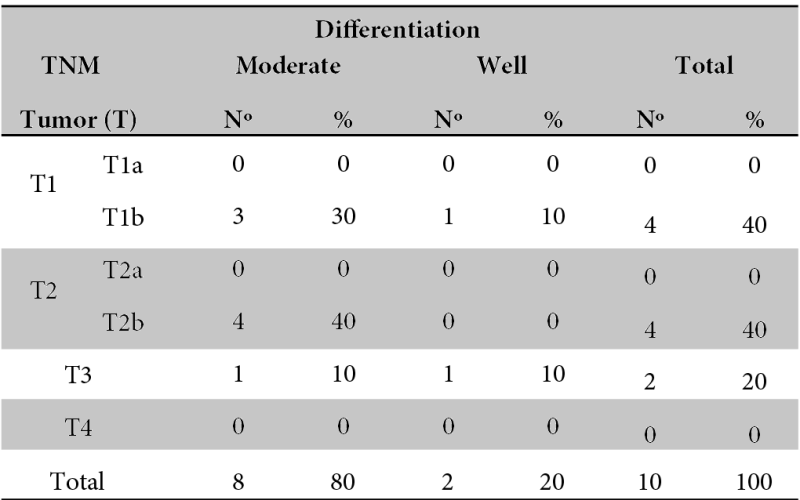
According to the TNM System (2018), 40% of patients were classified as T1b (30% moderately and 10% well differentiated); 40% as T2b (all moderately differentiated); and 20% as T3 (Table 1). There were no cases with lymph node involvement (N0) or distant metastases (M0).
In all cases a history of gallbladder lithiasis was collected, which was corroborated at the time of macroscopic examination of the surgical specimen or during necropsy.
Discussion
Gallbladder cancer is usually a pathology that, due to its clinical presentation, is confused with benign diseases of the gallbladder and this is usually related to the symptoms most frequently associated with the presence of gallbladder cancer and common to other conditions, such as colicky pain towards the right upper quadrant of the abdomen, jaundice, anorexia or hyporexia and weight loss.
According to the results of this study, a preoperative diagnosis of acute calculous cholecystitis was made in all patients studied by cholecystectomy biopsy, except in one patient where a clinical diagnosis of gallbladder cancer was made as a conclusion of the studies for jaundice; The three cases with necrotic findings of gallbladder cancer did not have a clinical diagnosis of gallbladder cancer, which may be directly related to the scarce radiological studies performed on the patients, since according to reports in the literature, the increase in the percentage of preoperative diagnosis is due to the combination of ultrasonography and tomography studies13.
The frequency of gallbladder cancer was 0.23% of malignant tumours, which, in comparison with other series, is well below that reported in world statistics, which range from 2.1% to 8.8%10,14and some other series have reported prevalence of 2.6%13. Gallbladder cancer has a worldwide incidence of 0.7% among malignant neoplasms. In the USA, the incidence is estimated at 1.2 cases per year15. In Argentina, there is a higher incidence in the northern provinces (Salta) of 6.7 per 100,000 inhabitants16. According to GLOBOCAN 2012 data, in Bolivia, CVB ranks fourth in terms of mortality by type of cancer.
Thus, the frequency of CVB in the “Joaquín Albarrán’’ Surgical Clinical Hospital is low compared to the prevalence in Chile, where high rates of CVB are reported.
Risk factors such as female sex and the presence of multiple vesicular lithiasis were evident in all the cases reported in this study, which corresponds to numerous case-control studies that have found associations with biliary pathologies and female sex as risk factors.
The female to male ratio is 3 to 4:110. The incidence for females in the USA is 1.45/100,000 inhabitants; in Chile it is 25.3/100,000 inhabitants17; in Bolivia the female-to-male ratio is 2.8:1 and in Colombia 2.2:118. In the study by Peña et al19. conducted in 3 referral hospitals in Chiclayo (Peru), CVB was found to occur in 72.4% women and 27.6% men; and in the study by Llanos et al20. 71.1% were found to be female and 28.9% male, showing a ratio of 3.5:1.
With regard to age, the results obtained in this study correspond to those described in the literature, which states that the mean age of presentation varies between 60 and 70 years, with presentation in people under 30 years of age being rare21.
In this study, there was no case of gallbladder calcification (porcelain gallbladder or hyaline calcinosis), which is associated with CVB in 10-25% of cases; calcification is considered the final stage of a chronic inflammatory process15,22. Other studies suggest that the reported incidence of cancer in patients with porcelain vesicles is between 10% and 20%. However, it would appear that the pattern of calcification is the most important feature, with focal mucosal calcification being the highest risk over diffuse transmural calcification23.
Other risk factors could not be ascertained, such as identification of Helicobacter bile and Pylori in bile specimens, which have been isolated from bile samples, suggesting an association with CVB1.
None of the cases had biliary polyposis, which is an important risk factor reported in the literature, detailing that the presence of solitary, asymptomatic polyps larger than 10 mm represents an increased risk of CVB24.
In this study, all cases were histologically adenocarcinoma (20% well-differentiated and 80% moderately differentiated). This, together with the degree of tumour infiltration, are factors influencing 5-year survival in patients with gallbladder cancer25. In one individual, infiltration to the liver bed without metastatic lesions could be confirmed.
The fact that all the tumours found in this study were adenocarcinoma corresponds to reports in the world literature which describe adenocarcinoma (papillary, tubular, mucinous or signet ring subtypes) as accounting for 80-95% of cases; epidermoid and adenosquamous carcinoma for 2-10%; undifferentiated carcinoma and other neoplasms (small cell carcinoma, sarcomas, melanomas and lymphomas) for only 2-7%26. Similar results were obtained in the study by Pina et al27 in which 94.1% of adenocarcinomas were found; and in the study by Peña et al.19 the predominant variety was adenocarcinoma in 82.8% of cases (mucinous carcinoma 5.2%).
Conclusion
Gallbladder cancer is a very rare disease and its diagnosis remains incidental, i.e. the diagnosis is established on histopathological examination after cholecystectomy or at necropsy. The most frequent variety is moderately differentiated adenocarcinoma.
References
1. Uribe MM, Heine TC, Brito MF, Bravo LD. Actualización en cáncer de vesícula biliar. Rev. Med. Clin. Condes - 2013; 24(4) 638-643. Available at: https://www.clinicalascondes.cl/Dev_CLC/media/Imagenes/PDF%20revista%20m%C3%A9dica/2013/4%20julio/9_Dr.-Mario-Uribe-M.pdf
2. Randi G, Franceschi S, La Vecchia C. Gallbladder cancer worldwide: geographical distribution and risk factors. Int J Cancer. 2006;118(7):1591–1602. Available at: https://onlinelibrary.wiley.com/doi/full/10.1002/ijc.21683
3. Lazcano-Ponce EC, Miquel JF, Muñoz N, Herrero R, Ferrecio C, Wistuba II, et al. Epidemiology and molecular pathology of gallbladder cancer CA Cancer J. Clin., 2001;51 (6):349-364. Available at: https://onlinelibrary.wiley.com/doi/full/10.3322/canjclin.51.6.349?sid=nlm%3Apubmed
4. Gamarra RR, Coapaza Y, Salazar F, Ojeda Y. Cáncer de vesícula biliar según tipo histológico y clasificación TNM en Arequipa, Perú. Acta Med Per. 2012;29(1):23–7. Available at: http://www.scielo.org.pe/pdf/amp/v29n1/a09v29n1.pdf
5. Ministerio de Salud Pública. Anuario Estadístico de Salud 2018. La Habana-Cuba 2019. http://files.sld.cu/bvscuba/files/2019/04/Anuario-Electr%C3%B3nico-Espa%C3%B1ol-2018-ed-2019-compressed.pdf
6. Kumar V, Abbas AK, Fausto N, Aster JC. Robbins y Cotran Patología estructural y funcional Novena edición. 2010 Elsevier España, S.L. 879-880
7. Izarzugaza M, Fernández L, Forman D, Sierra M. Burden of gallbladder cancer in Central and South America. Cancer Epidemiology 2016;44(1):S82-S89. Available at: https://www.sciencedirect.com/science/article/pii/S1877782116301163
8. Andia ME, Hsing AW, Andreotti G, Fereccio C. Geographic variation of gallbladder cancer mortality and risk factors in Chile: a population-based ecologic study. Int J Cancer. 2008;123(6):1411–1416. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2864002/
9. De Aretxabala X. Cáncer de vesícula biliar. Consideraciones luego del consenso. Rev Chil Cir. 2007;59:472-474. Available at: https://scielo.conicyt.cl/pdf/rchcir/v59n6/art16.pdf
10. Campos YM, Brenes I. Cáncer de vesícula biliar. Rev Med de Costa Rica y Centroamérica 2008; 65(583): 147-152. Available at: https://www.medigraphic.com/pdfs/revmedcoscen/rmc-2008/rmc082m.pdf
11. Giang TH, Ngoc TT, Hassell LA. Carcinoma involving the gallbladder: A retrospective review of 23 cases-Pitfalls in diagnosis of gallbladder carcinoma. Diagn Pathol. 2012, 7.10:1-8. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3285085/
12. Chan CP, Chang HC, Chen YL, Yang LH, Chen ST, Kuo SJ, et al. A 10-year experience of unsuspected gallbladder cancer after laparoscopic cholecystectomy. Int Surg. 2003; 88: 175-179. https://www.ncbi.nlm.nih.gov/pubmed?db=PubMed&cmd=Retrieve&list_uids=14584775
13. Castillo JJ, Romo C, Ruiz J, Escrivá JF, Córdova VH. Cáncer de vesícula biliar como hallazgo histopatológico posterior a la colecistectomía. Prevalencia e incidencia en el Hospital Ángeles Pedregal. Acta Med Grupo Ángeles. 2010;8(3). https://www.medigraphic.com/pdfs/actmed/am-2010/am103c.pdf
14. Roa I, Guzmán P, Ibacache TM, Araya J, Villaseca M, De Aretxabala X, et al. Cáncer de la vesícula biliar en colecistectomías por litiasis. Rev Esp Patol 2004; 37(3): 279-285. Available at: http://www.patologia.es/volumen37/vol37-num3/37-3n06.htm
15. Chan NC, Bandín MA, Villalobos BI, Torres MA. Guía de práctica clínica. Cáncer de vesícula biliar. Asociación Mexicana de Cirugía General, A.C. Guías de Práctica Cínica. México. 2014. Available at: https://amcg.org.mx/images/guiasclinicas/cancer_vesicular.pdf
16. Ledndoire J, Gil L. Carcinoma de la vesícula biliar. Enciclopedia Cirugía Digestiva. F. Galindo y colab. Sociedad Argentina de Cirugía Digestiva. 2015; tomo IV-463:1-22. Available at: http://www.sacd.org.ar/ccuatrosesentaytres.pdf
17. Hueman M, Vollmer C, Pawlik T. Evolving treatment strategies for gallbladder cancer. Annals of surgical oncology. 2009;16(8):2101–15. Available at: http://dx.doi.org/10.1245/s10434-009-0538-x.https://www.ncbi.nlm.nih.gov/pubmed/19495882
18. Wernberg JA, Lucarelli DD. Gallbladder cancer. Surg Clin North Am. 2014;94(2):343-60. Available at: https://www.sciencedirect.com/science/article/pii/S0039610914000103?via%3Dihub
19. Peña F, Sánchez F. Frecuencia y perfil clínico de cáncer de vesícula biliar en pacientes colecistectomizados en 3 Hospitales Referenciales de Chiclayo entre 2011 Y 2016. [Tesis de Grado]. Universidad Católica Santo Toribio de Mogrovejo. Chiclayo. 2018. Available at: https://pdfs.semanticscholar.org/6bce/f78ccfd1f5dea87187aa5d77277be6d5f766.pdf
20. Llanos F José Luis, Trujillo Carlos, Zilvetty P Emma. ESTUDIO CLÍNICO - PATOLÓGICO DEL CÁNCER DE VESÍCULA BILIAR EN 33 AÑOS INSTITUTO GASTROENTEROLÓGICO BOLIVIANO JAPONÉS. Revista Científica UNITEPC [revista en la Internet]. 2011 Nov [citado 2020 Jul 24]; (1): 12-20. Available at: http://www.revistasbolivianas.org.bo/scielo.php?script=sci_arttext&pid=S2124-10112011000100003&lng=es
21. Arroyo G. Cáncer de vesícula biliar. Oncol. Clin. 2002;8(1):831-837.
22. Baca JE, Magaña J. Vesícula biliar “en porcelana”. Acta Médica Grupo Ángeles. 2018; 16(3). Available at: https://www.medigraphic.com/pdfs/actmed/am-2018/am183o.pdf
23. Hepp J, Lo C. Gallbladder Cancer. In: Clavien PA, editor. Malignant Liver Tumors: Current and Emerging Therapies. 3rd ed. Editado por Pierre-Alain Clavien.© por Blackwell Publishing 2010: 333–41. Available at: http://the-eye.eu/public/Books/Medical/texts/Malignant%20Liver%20Tumors%20-%20Current%20and%20Emerging%20Therapies%203rd%20ed%20-%20P.%20Clavien%20%28Wiley-Blackwell%2C%202010%29%20WW.pdf
24. Dutta U. Gallbladder cancer: can newer insights improve the outcome? Journal of gastroenterology and hepatology [Internet]. 2012;27(4):642–53.Available at: https://www.ncbi.nlm.nih.gov/pubmed/22168580
25. Ramírez CP, Suárez MA, Santoyo J, Fernández JL, Jiménez M, Pérez JA, et al. Actualización del diagnóstico y tratamiento del cáncer de vesícula biliar. Cir Esp 2002; 71(2):102-111. Available at: https://www.elsevier.es/es-revista-cirugia-espanola-36-articulo-actualizacion-del-diagnostico-el-tratamiento-S0009739X02719404
26. Calderillo-Ruiz G, Herrera-Goepfert R, Díaz-Romero C, Carbajal-López B, López-Basave H. Carcinoma epidermoide puro-combinado de vesícula biliar. Rev. Méd. Chile. 2018;146(12). Available at: http://dx.doi.org/10.4067/s0034-98872018001201438.
27. Pina L, Lagos H, Quiche G, Alle L, Sarotto LE. carcinoma incidental de vesícula biliar en un hospital universitario. Acta Gastroenterol Latinoam 2017;47(3):190-193. Available at: http://www.actagastro.org/numeros-anteriores/2017/Vol-47-N3/Vol47N3-PDF08.pdf
Author notes
E-mail: b51amazonas@gmail.com
Conflict of interest declaration
Alternative link

